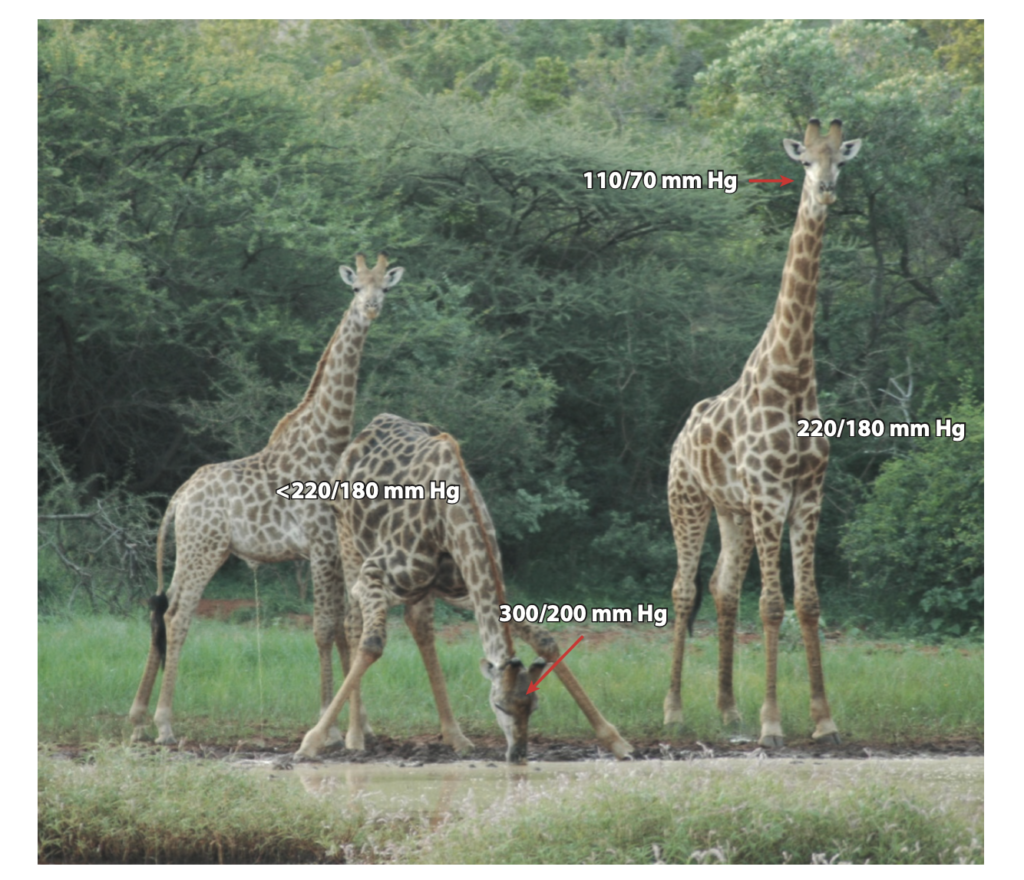
Illustration of the blood pressure and arterial pressures in the heads of giraffes in different positions. In particular, the arterial pressure in the head of a drinking giraffe is only reported for one animal and needs confirmation. Note that information on aspects of water homeostasis of giraffes is also apparent from the figure. References: The Remarkable Cardiovascular System of Giraffes. Annu.Rev.Physiol.2021.83:1–15
The remarkable value of the dysautonomia field study in Mexico
- Conditions associated with autonomic dysfunction (another term for dysautonomia) are common and are observed daily in medical consultations in every medical office across our country.
- “Dysautonomia is a term that physicians often use as a diagnostic conclusion to describe a set of diffuse and vague symptoms (primarily due to orthostatic intolerance). However, the term is not specific to any particular condition, as multiple disorders can present with the same symptoms [1].”
- “The clinical evaluation of dysautonomia has evolved significantly over the past four decades. It is based on increasingly sophisticated methods for quantifying and observing common physiological variables (blood pressure and heart rate). These advances allow for greater diagnostic precision, a deeper understanding of autonomic physiology, and truly individualized treatment adjustments for each patient [2].”
- “While a thorough clinical history is the most important tool for suspecting dysautonomia” (in the words of Dr. Goldstein, a pioneer in the autonomic field), it requires patience, time, and a precise focus on the symptoms reported by the patient. These symptoms can be vague and confusing and are frequently exacerbated by anxiety, depression, difficulty falling asleep, dehydration, cognitive and emotional stress, environmental factors, medications, and others. The physician must therefore dedicate at least 60 minutes to the patient interview and formulate targeted questions to detect symptoms of dysautonomia [3].”
- In Mexico, the in-depth study of these conditions is particularly remarkable in certain cases, such as hereditary transthyretin (TTR) amyloidosis, which causes abnormal deposition of the protein encoded by the mutated gene in peripheral nerves and other organ systems. Research conducted by pioneers in the field helps us understand how this condition is distributed in the Mexican population and allows us to offer targeted treatments to these patients, who previously lacked effective therapeutic options. Today, available treatments can achieve remission of the disease [4].
- “However, there are multiple conditions that affect the function of the baroreceptors involved in the delicate systems controlling blood pressure and heart rate. These conditions must be properly classified and characterized to provide each patient with the correct diagnosis and individualized therapeutic options.”
- “To understand man, it is necessary to understand culture” is an adaptation of a famous phrase by Napoleon Bonaparte. Therefore, to understand dysautonomia, it is essential to comprehend the specific characteristics of a population as complex as that of our country.”
- “Our project provides patients and their referring physicians with highly precise diagnoses by combining international-standard evaluations performed in prestigious centers in the United States and around the world, with a distinctive ‘Mexican-style’ adaptation. This dynamic evaluation of each patient’s physiological parameters makes every assessment truly unique — because each person is unique in their blood pressure, heart rate, and response to cognitive, environmental, and emotional stress.”
- “We are excited to share this project with you, which opens a new door to the field of dysautonomia in Mexico and to its unique demographic characteristics worldwide.”
References
- Benarroch EE. “Dysautonomia”: a plea for precision. Clin Auton Res. 2021;31(1):27-29. doi:10.1007/s10286-020-00749-3
- O’Dell JA, Walker A, Latham AJ, Parisian DJ, Branch LE, Vanderburg DD, Cox AA, Chavis S, Smith SE. The Diagnostic Journey of Dysautonomia Patients: Insights from a Patient-Reported Outcome Study. J Patient Exp. 2025 Jan 21;12:23743735251314651. doi: 10.1177/23743735251314651.
- Novak, P., Systrom, D., Marciano, S.P. et al. Mismatch between subjective and objective dysautonomia. Sci Rep 14, 2513 (2024). https://doi.org/10.1038/s41598-024-52368-x
- González-Duarte A, Cárdenas-Soto K, Bañuelos CE, Fueyo O, Dominguez C, Torres B, Cantú-Brito C. Amyloidosis due to TTR mutations in Mexico with 4 distinct genotypes in the index cases. Orphanet J Rare Dis. 2018 Jul 3;13(1):107. doi: 10.1186/s13023-018-0801-y.
Our facilities in Mexico

*Establish the most comprehensive national registry of autonomic conditions (dysautonomias) in Mexican patients with sporadic, acquired, and genetic disorders of the autonomic nervous system.
*Create and run longitudinal follow-up of patients with autonomic dysfunction in degenerative brain diseases, both sporadic and hereditary (such as atypical Parkinsonism, hereditary ataxias, and Huntington’s disease, genetic pediatric and adult-onset leukodystrophies, among others).
*Collect and publish scientific information on the Mexican phenotype of patients with Pure Autonomic Failure (PAF) and other synucleinopathies.
*Describe the clinical phenotype in the functional neurological disorder found in Mexican patients, and its association with function afferent baroreceptor failure manifestations (vasovagal syncope, Postural Orthostatic Tachycardia Syndrome (POTS), and orthostatic intolerance) to establish strategies for baroreceptor rehab and physical reconditioning.
*Become a leading institution in Mexico and LATAM for all conditions associated with afferent and efferent baroreceptor failure.
*Compete in the immediate future with the leading autonomic research centers in the United States and around the world.
Timeline of Autonomic Evaluation in Mexico
Initial simplified Autonomic Evaluation
August 2025
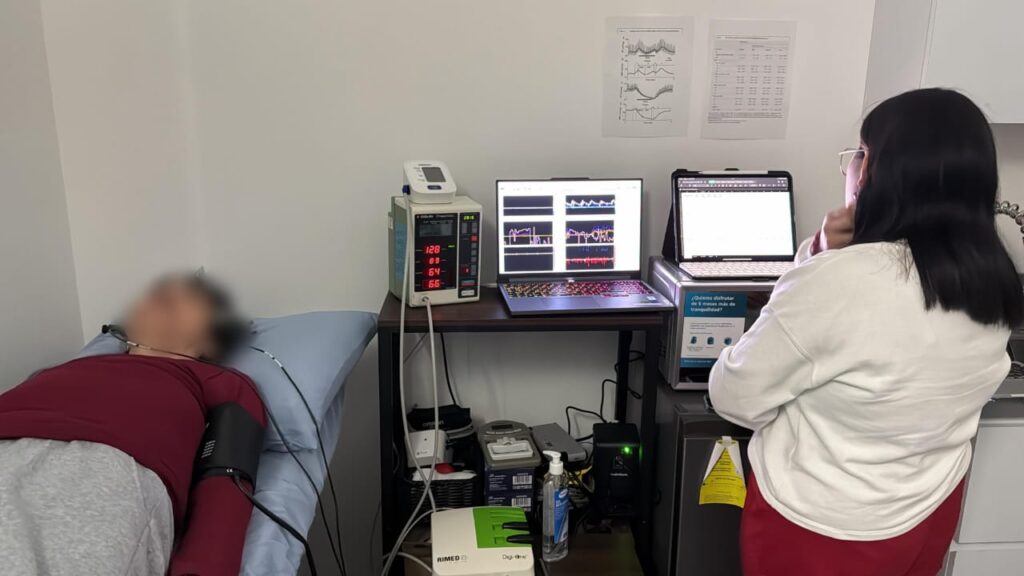
- First Autonomic Laboratory Foundation, Santa Fe Contadero, Mexico City.
- Initial evaluation of the blood pressure and pulse behaviors.
- Passive tilt table
- Assessment protocol
- Sitting
- First supine
- Phase 1 – Passive tilt
- Phase 2 – blood pressure challenges to evaluate pressor response to stressors.
- Second supine (recovery phase)
- Assessment protocol
- Passive tilt table
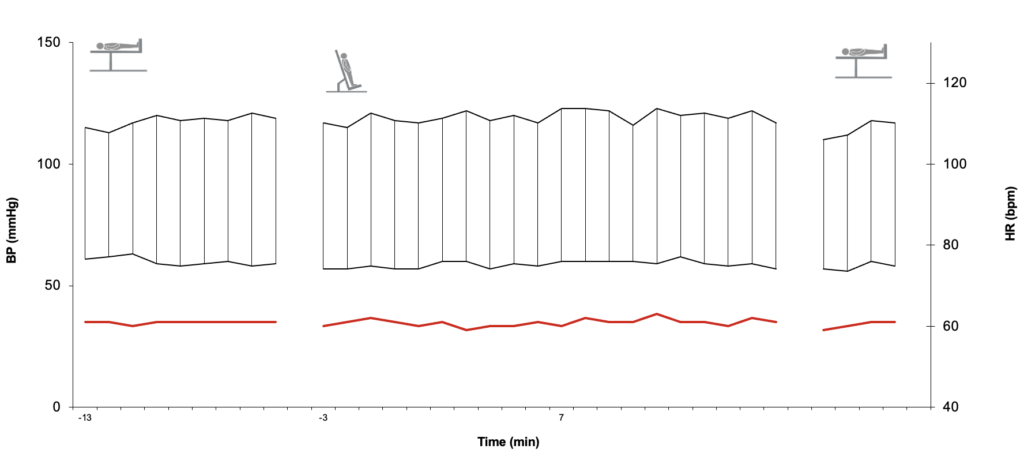
Example of a Healthy 70-Year-Old Man with Normal Baroreceptors in Response to Postural Changes (Initial Supine Position, Passive Tilt, and Supine Recovery Phase)
Autonomic assessment – 2 times
October, 2025
- Time 1.
- Sitting
- First supine
- Phase 1 – Passive tilt
- Phase 2 – blood pressure challenges to evaluate pressor response to stressors.
- Second supine (recovery phase)
- Time 2. Oral glucose challenge.
- Sitting
- First supine
- Phase 1 – Passive tilt
- Phase 2 – blood pressure challenges to evaluate pressor response to stressors.
- Second supine (recovery phase)
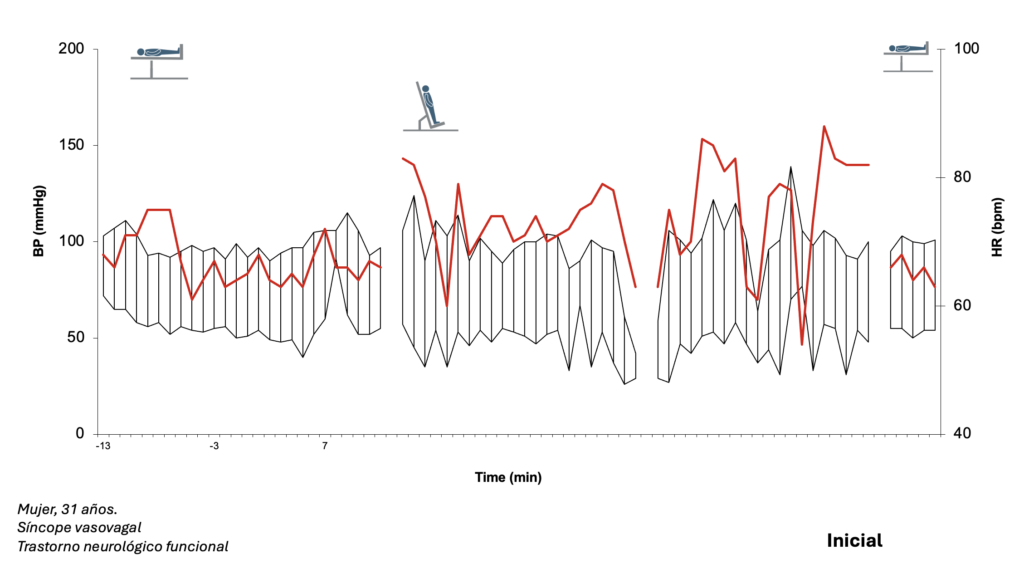
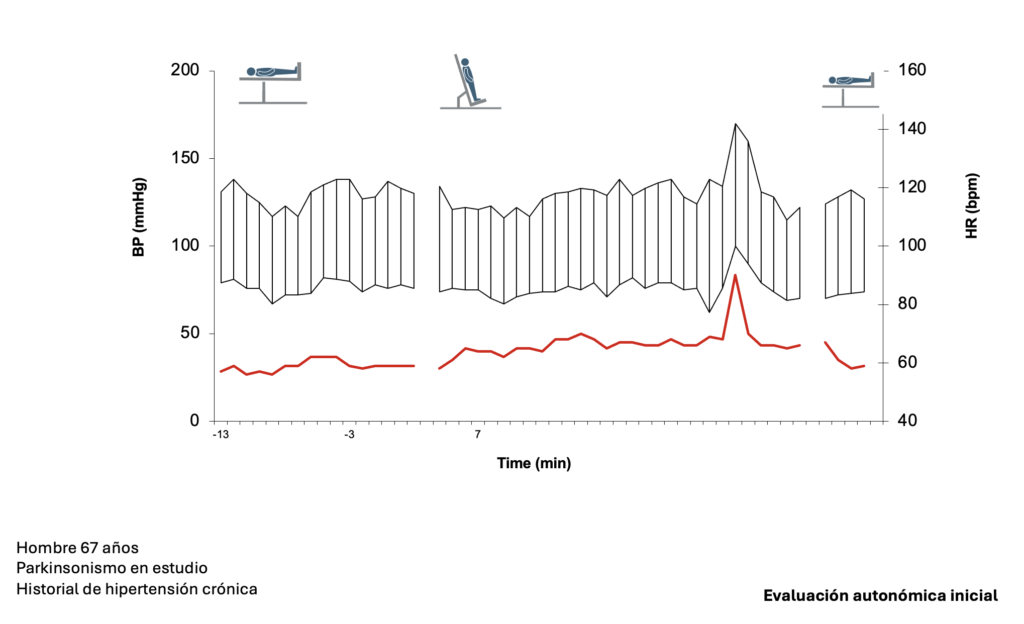
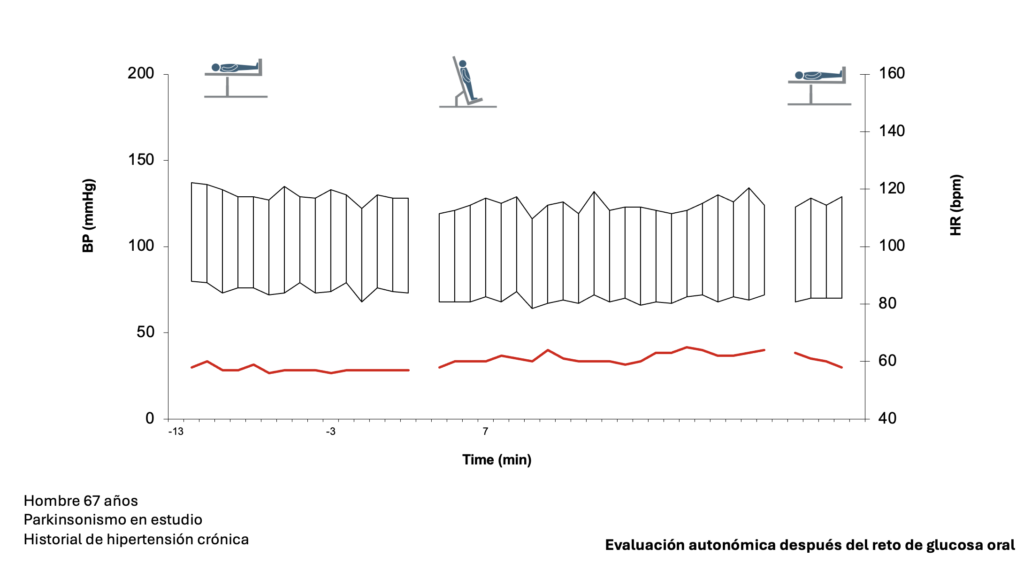
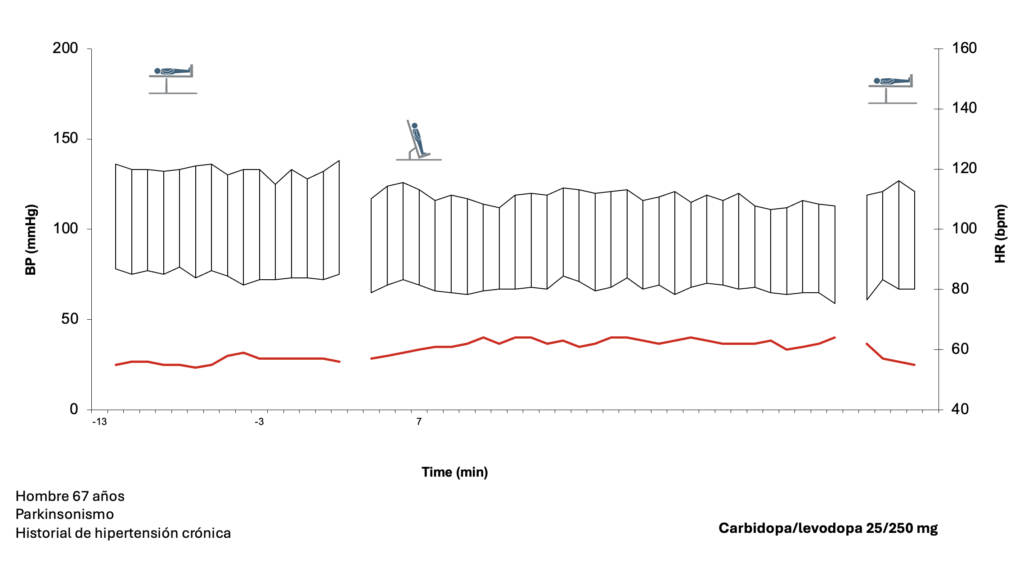
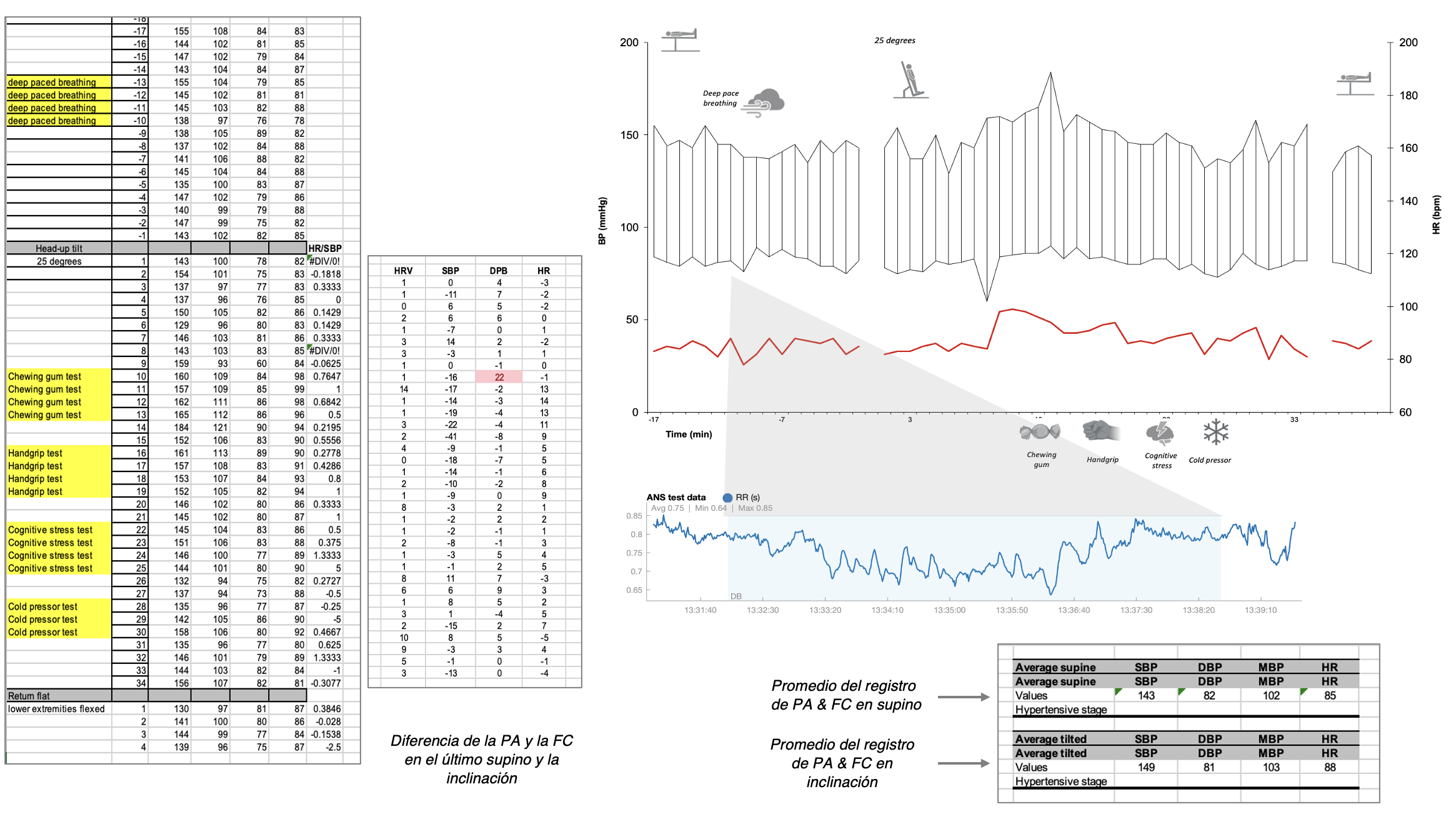
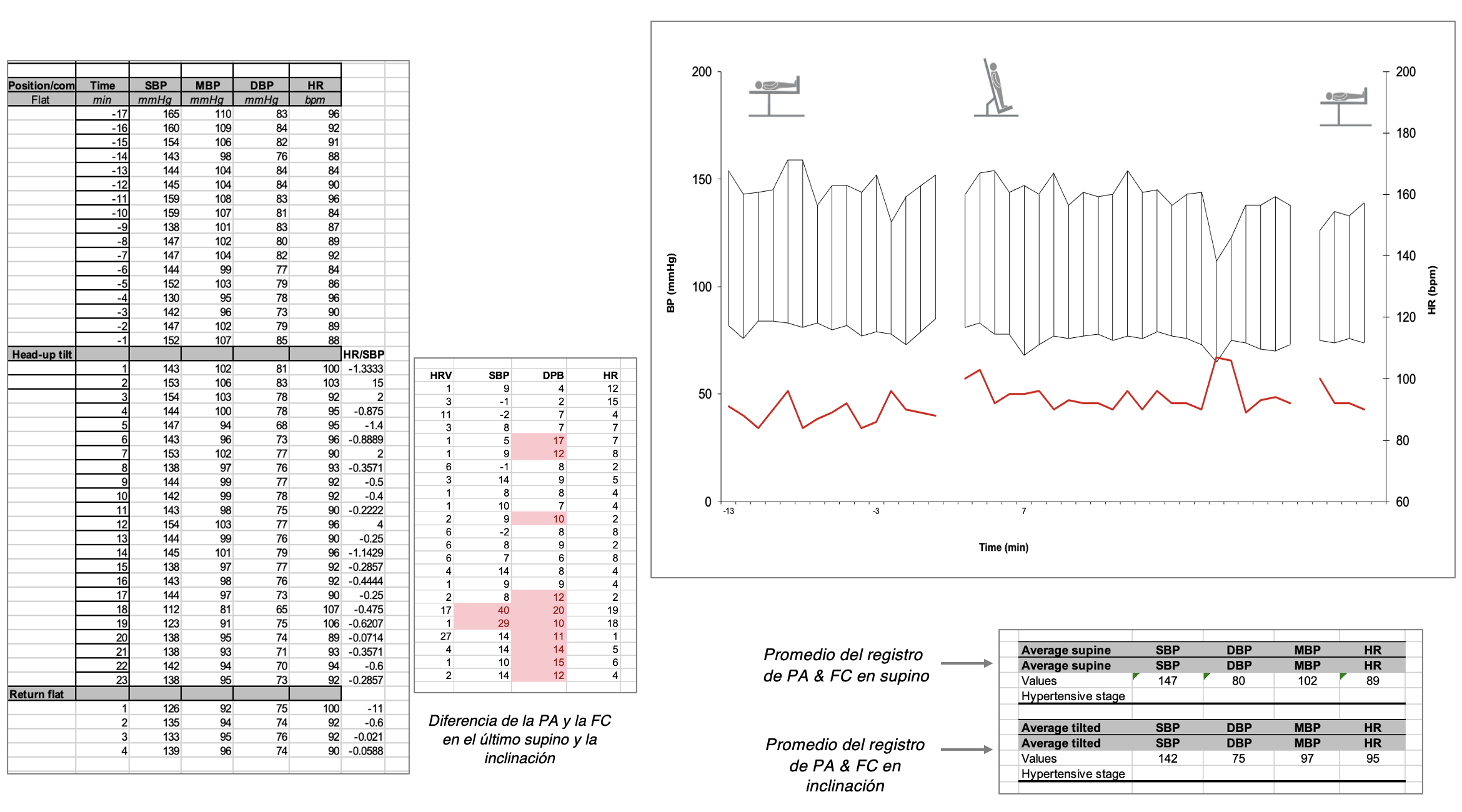
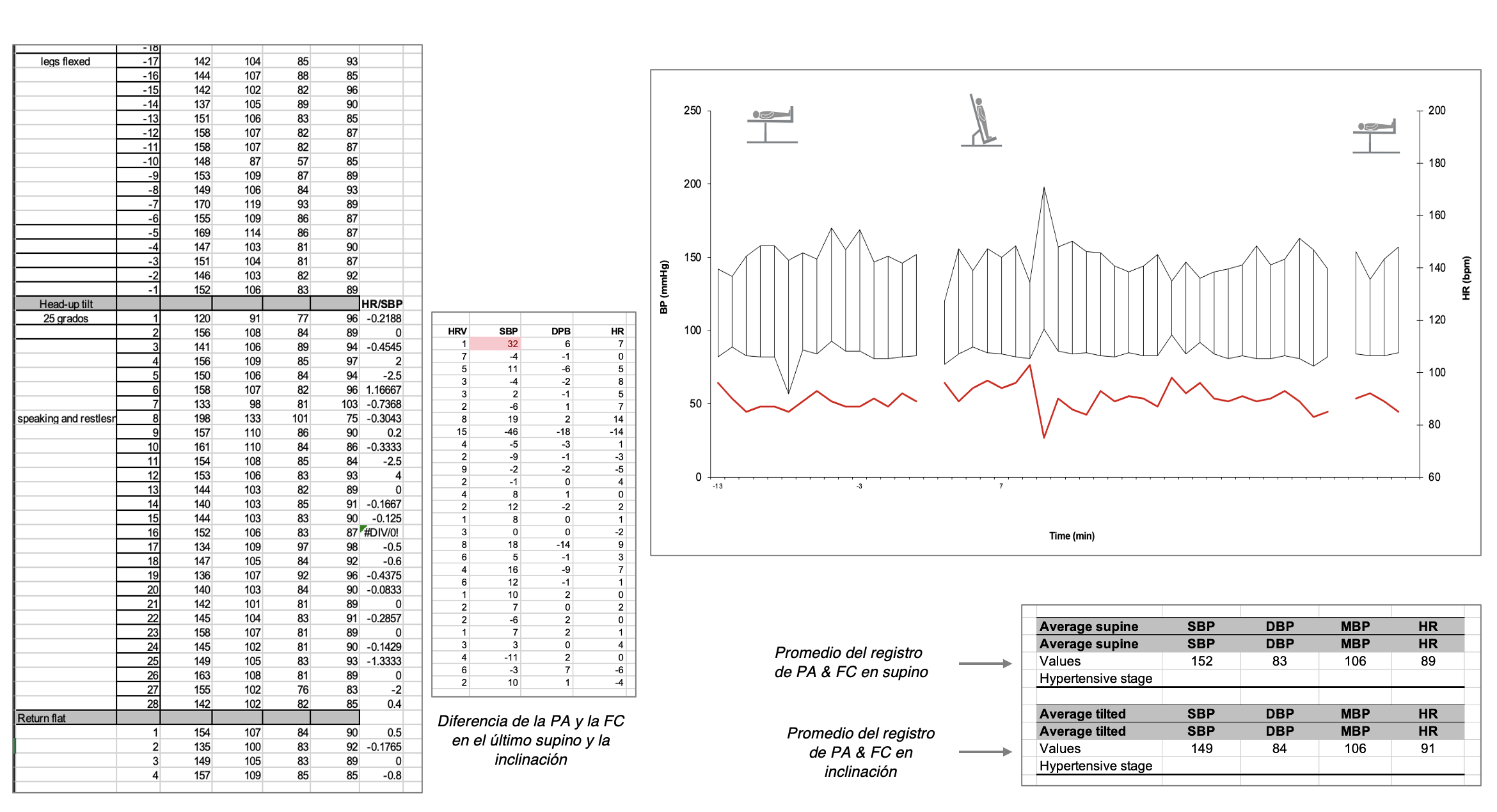
Ejemplos de evaluaciones autonómicas en pacientes con protocolo de 2 tiempos.
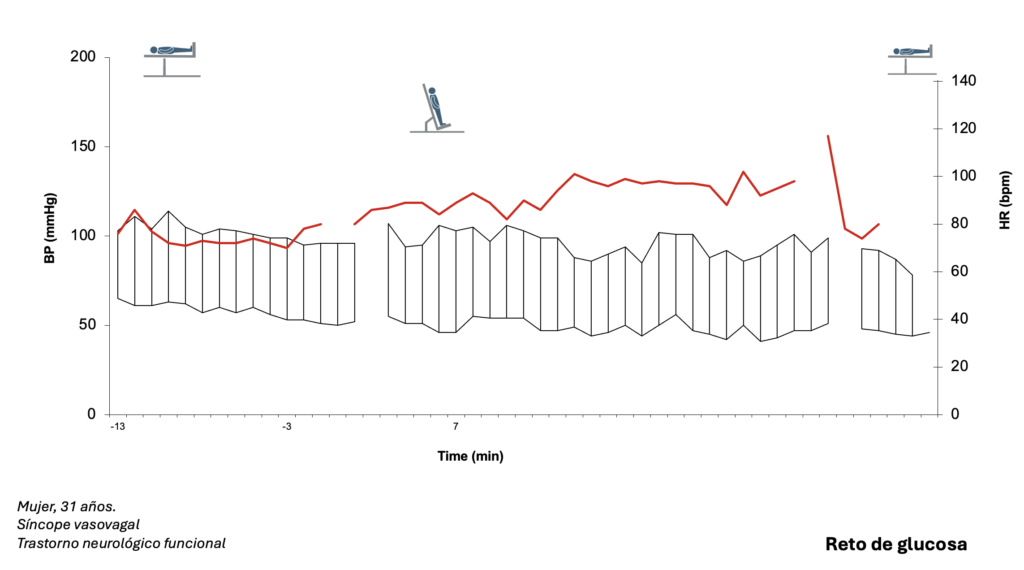
Evaluación autonómica – 3 tiempos
Noviembre 2025
- Evaluación inicial del comportamiento de la presión y el pulso durante la prueba de mesa inclinada
- Tiempo 1.
- Mesa inclinada pasiva
- Retos para evaluar la reacción de la presión arterial y el pulso (estándar)
- Tiempo 2. – Reto con glucosa oral
- Mesa inclinada pasiva
- Retos para evaluar la reacción de la presión arterial y el pulso (casos especiales)
- Tiempo 3. – Reto farmacológico individualizado
- Mesa inclinada pasiva
- Retos para evaluar la respuesta de la presión arterial y el pulso – (opcional)
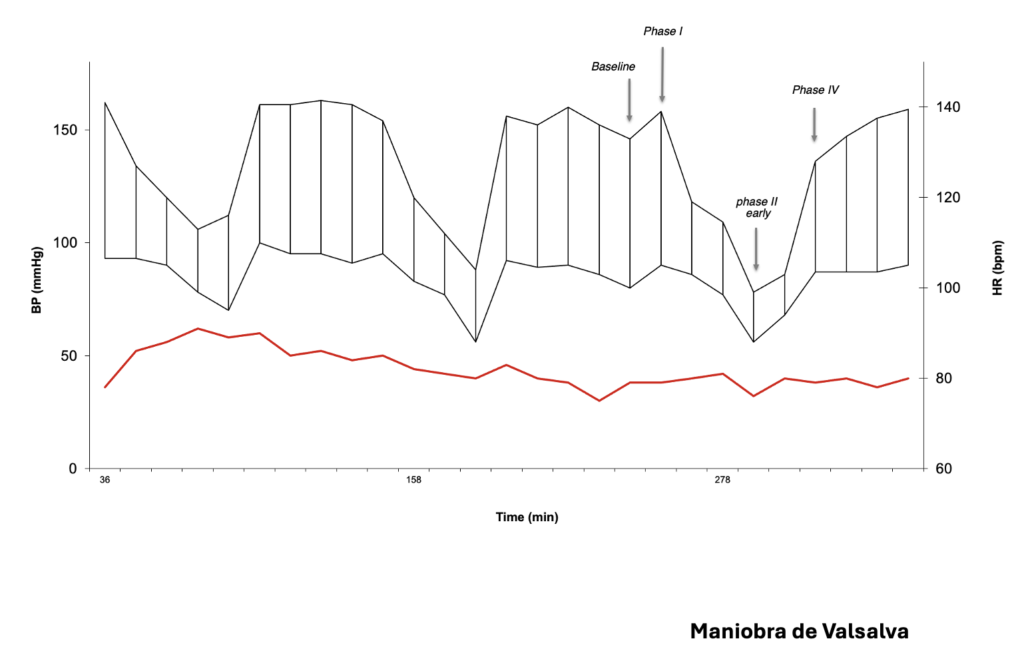
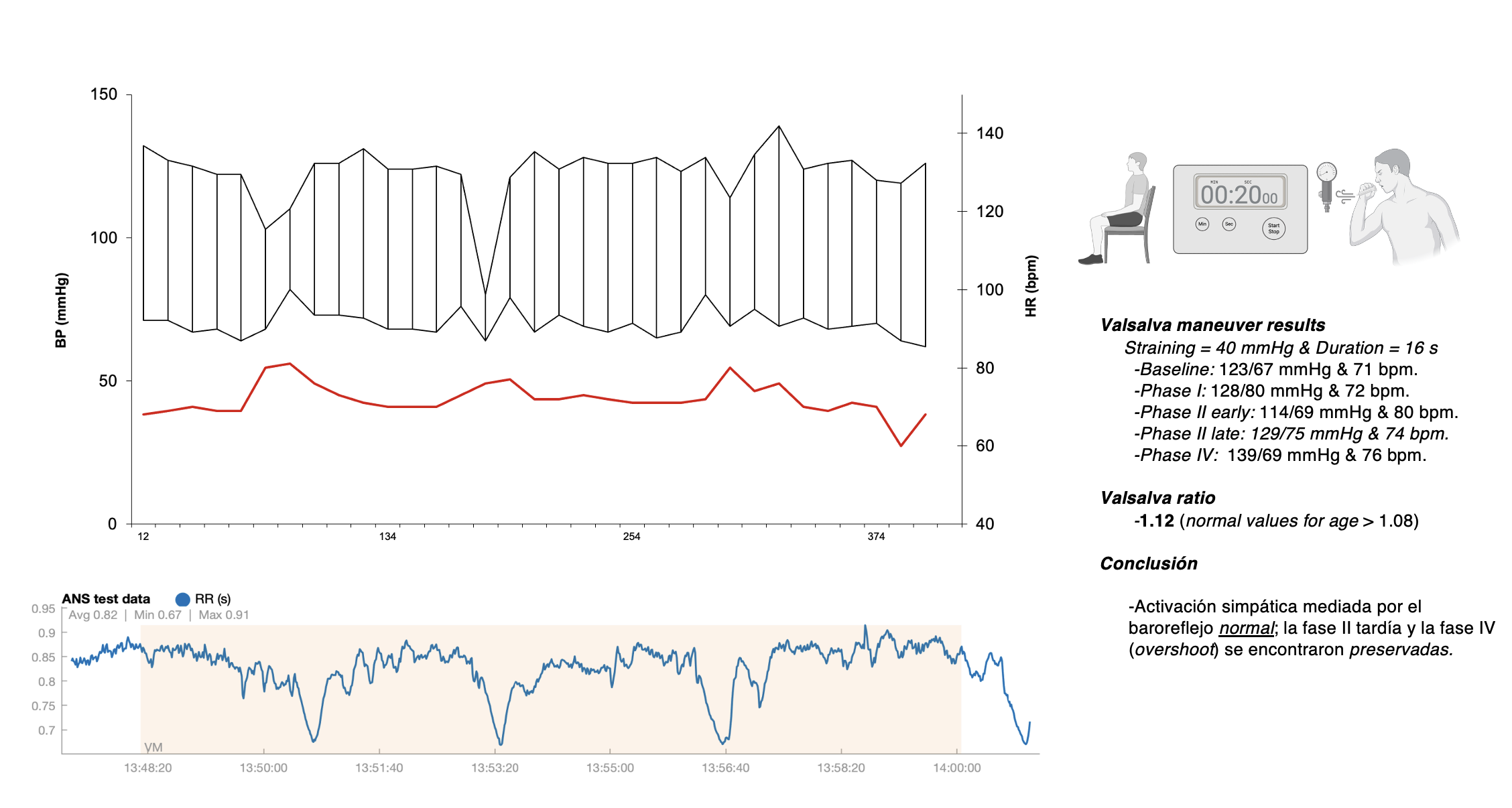
- Maniobra de Valsalva utilizando el sistema Colin Press Mate.
- Tiempo 1.
Ejemplos de evaluaciones autonómicas en pacientes con protocolo de tiempos.
Evaluación autonómica – 3 tiempos
Evaluación inicial del comportamiento de la presión y el pulso durante la prueba de mesa inclinada
Tiempo 1.
-Mesa inclinada pasiva
-Retos para evaluar la reacción de la presión arterial y el pulso (estándar)
Tiempo 2. – Reto con glucosa oral
-Mesa inclinada pasiva
-Retos para evaluar la reacción de la presión arterial y el pulso (individualizado)
Tiempo 3. – Reto farmacológico individualizado
-Mesa inclinada pasiva
-Retos para evaluar la respuesta de la presión arterial y el pulso (individualizado)
-Maniobra de Valsalva utilizando el sistema Colin Press MateR y el Kubios HRV SystemR
Ejemplo de evaluaciones autonómicas en pacientes con protocolo de tres tiempos
Febrero 2026
Evaluación autonómica de 3 tiempos & Colin Press Mate & Kubios System HRV & Cerebral Blood Flow &
Evaluación inicial del comportamiento de la presión y el pulso durante la prueba de mesa inclinada
Tiempo 1.
-Mesa inclinada pasiva
-Retos para evaluar la reacción de la presión arterial y el pulso (estándar)
-Ultrasonido Doppler transcraneal durante todo el primer tiempo***.
Tiempo 2. – Reto con glucosa oral
-Mesa inclinada pasiva
-Retos para evaluar la reacción de la presión arterial y el pulso (individualizado)
Tiempo 3. – Reto farmacológico individualizado
-Mesa inclinada pasiva
-Retos para evaluar la respuesta de la presión arterial y el pulso (individualizado)
-Maniobra de Valsalva utilizando el sistema Colin Press MateR y el Kubios HRV SystemR
***Inicio de pruebas en pacientes selectos.
Ejemplos de evaluaciones autonómicas con monitoreo del flujo sanguíneo cerebral
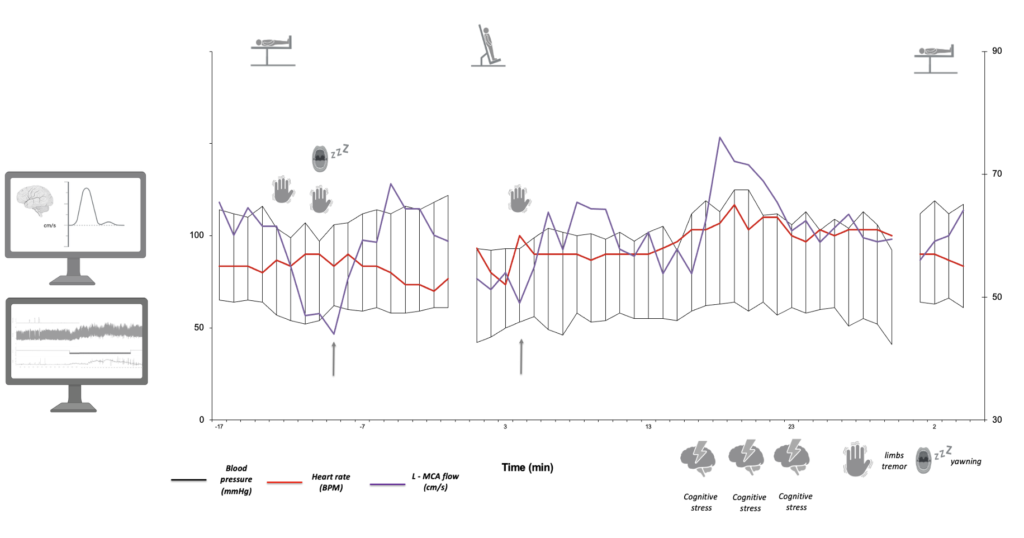
Masculino de 70 años. Parkinsonismo degenerativo – medicamento OFF
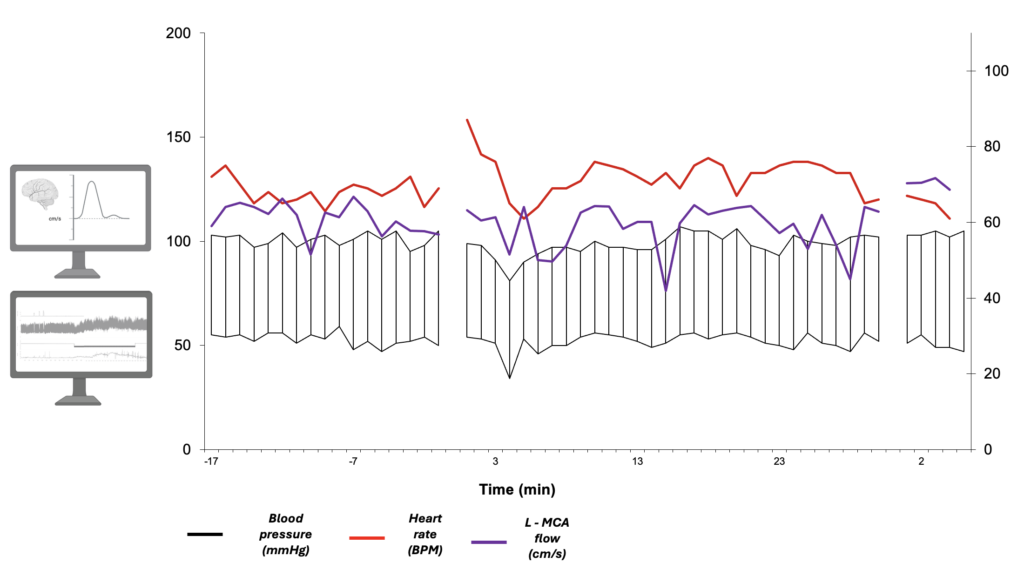
Masculino de 28 años. Sincope vasovagal neural-mediado.